When you go to the hospital to have yourself checked, get admitted, or just for medical employment purposes, it is not the doctor that you see first. The nurses would have to attend to you first before you get to see the doctor. The nurses then do what is called a nursing assessment. This assessment usually includes your height measurement, weight measurement, temperature, blood pressure, heart rate, and respiratory rate. For medical employment purposes, an eye examination is included to this assessment.
Nursing assessment forms vary depending on the institution or hospital. We have nursing assessment sample forms below for you to view or download. We also have other Sample Forms that you may find helpful.
Sample Pediatric Nursing Assessment Form
Nursing Health Assessment Form in PDF
Nursing Patient Assessment Form
Comprehensive Nursing Assessment Form
Types of Nursing Assessment
- Initial Assessment
The initial assessment is the first assessment done by the nurse and is also called triage. It is a thorough assessment that helps determine the problem and helps in the preparation of further assessments. The initial assessment includes taking of the vital signs, patient’s health history, family health history, and the patient’s chief complaint. We have Physical Assessment Forms that are also used during an initial assessment.
- Focused Assessment
This type of assessment includes lab tests, like X-ray tests. A focused assessment is done when a the problem is already identified. Nurses also use this assessment to determine if the problem still exists, is resolved, or has worsened. The goal of this assessment is to stabilize the patient’s health condition.
- Time-Lapsed Assessment
The time-lapsed assessment is done after the initial assessment to evaluate any changes in the patient’s health. This is done two or three hours after the initial assessment or in a couple of months depending on the patient’s condition.
- Emergency Assessment
This type of nursing assessment is used during life-threatening situations wherein time is of the essence and the preservation of the patient’s life is a priority. It utilizes the ABCs of the nursing assessment.We also have other assessment forms available, like the Training Assessment Forms.
Nursing Admission Shift Assessment Form
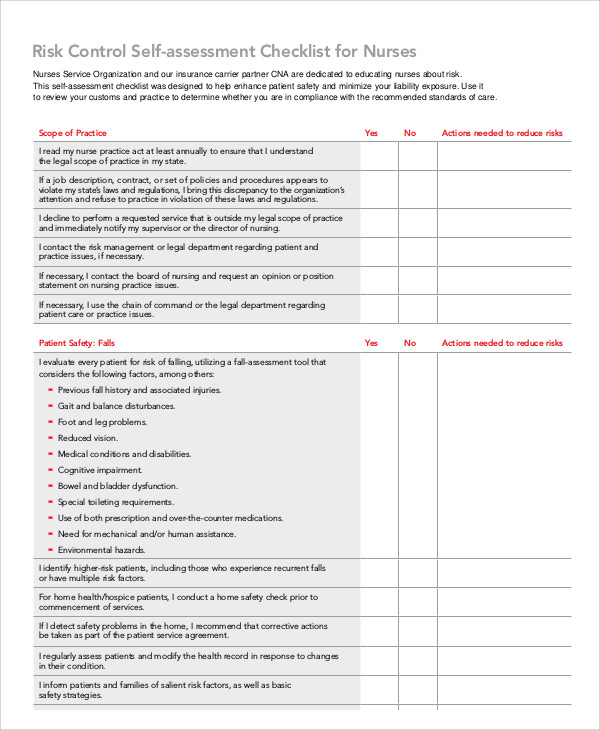
Nursing Self-Assessment Checklist Form
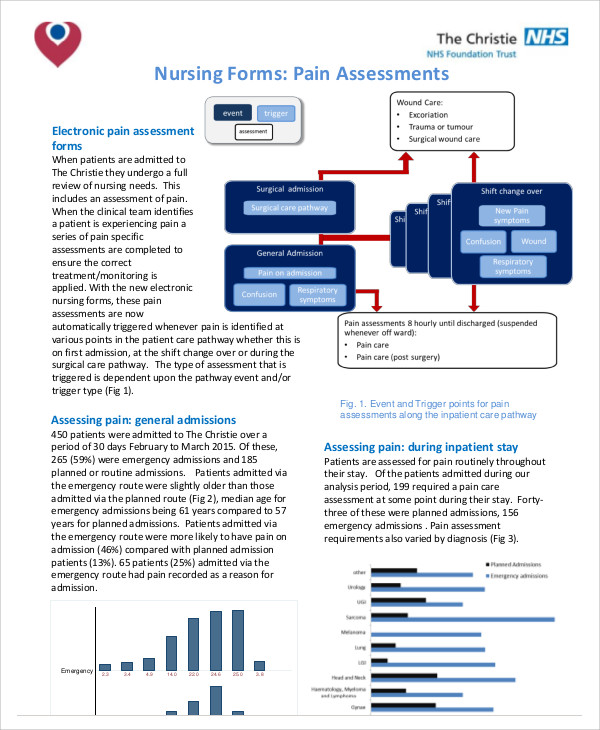
Nursing Pain Assessment Form
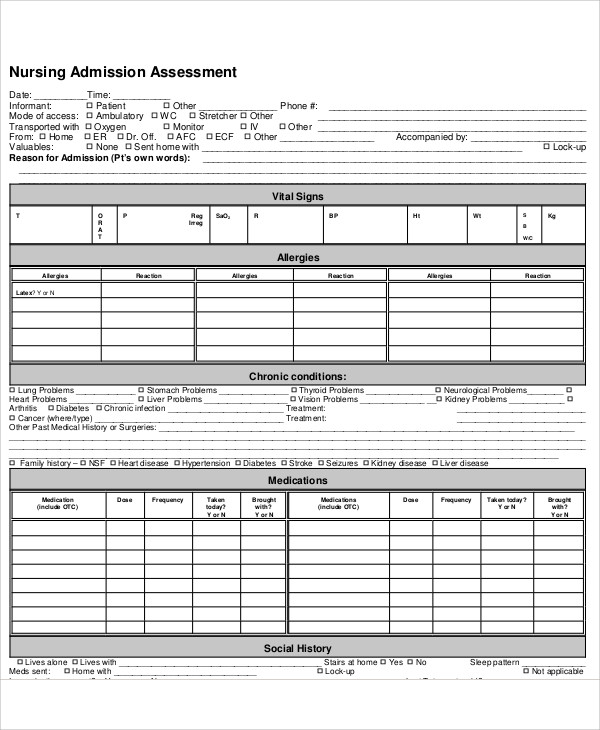
Nursing Admission Assessment Form
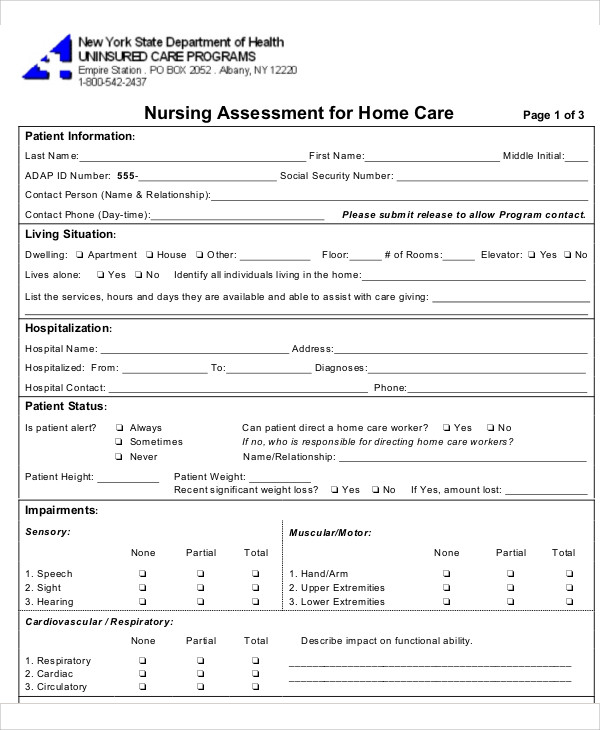
Home Care Nursing Assessment Form
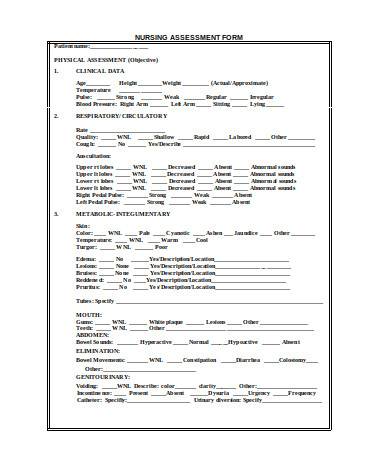
General Nursing Assessment Form
The Purpose of a Nursing Assessment
It is specifically called a nursing assessment because the doctors also have their own assessments to do. It limits the things that the nurses can assess and at the same time prepares valuable information to the doctor about the patient before meeting them. Some doctors don’t know how to perform most of the assessments that the nurses do and others just tend to have the nurses do it for them. The nursing assessment allows the nurse to thoroughly check the patient so that they can determine what kind of doctor they initially send the patient to.
In the hospital setting, having the nurses asses the patient before they see the doctor helps in speeding up the checkup process, especially when there are a lot of patients in queue. Nurses who perform assessments during emergency situations can also save lives in cases where a doctor is not within the vicinity. Another purpose of the nursing assessment is to monitor the changes in the health condition of both long-term and short-term patients in the hospital.
Whatever your purpose is for doing a nursing assessment, these nursing assessment sample forms will definitely be of use to you. You may also find our Fitness Assessment Forms useful. So don’t leave without downloading!
Related Posts
Sample Sworn Affidavit Forms
Vehicle Inspection Forms Samples & Templates
Sample Employee Advance Forms
Sample Child Travel Consent Forms
Sample Testimonial Request Forms
Sample Employee Details Forms
Sample Divorce Forms
Sample Attestation Forms
Employee Performance Appraisal Form Templates
FREE 9+ Sample Presentation Evaluation Forms in MS Word
FREE 10+ School Admission Form Samples & Templates in MS Word | PDF
FREE 30+ Patient Consent Form Samples in PDF | MS Word
FREE 10+ Sample Sign Off Form Templates in PDF | MS Word
FREE 11+ Sample Medical Consultation Forms in PDF | MS Word
FREE 8+ Sample Donation Forms in PDF | MS Word