
A “brain sheet”, often and professionally referred to as Nurse Sheet is simply a reference used by nurses so they can keep track of important information about each patient that they are handling. This sheet is often filled out with key information during change-of-shift report and then updated as things change especially on major problems and events that could happen to the patient anytime under the care of the nurse. The sheet is then used at the end of shift to give sample report and note to the oncoming nurse, this makes a good brain sheet key for patient safety and effective communication, a thing considered achievement for nurses. If you are interested in availing samples of Nursing Report Sheet or any other reports, you may want to browse through this article and make use the available templates provided.
A “brain sheet”, often and professionally referred to as Nurse Sheet is simply a reference used by nurses so they can keep track of important information about each patient that they are handling. This sheet is often filled out with key information during change-of-shift report and then updated as things change especially on major problems and events that could happen to the patient anytime under the care of the nurse. The sheet is then used at the end of shift to give sample report and note to the oncoming nurse, this makes a good brain sheet key for patient safety and effective communication, a thing considered achievement for nurses. If you are interested in availing samples of Nursing Report Sheet or any other reports, you may want to browse through this article and make use the available templates provided.
11+ Nursing Report Sheet Samples
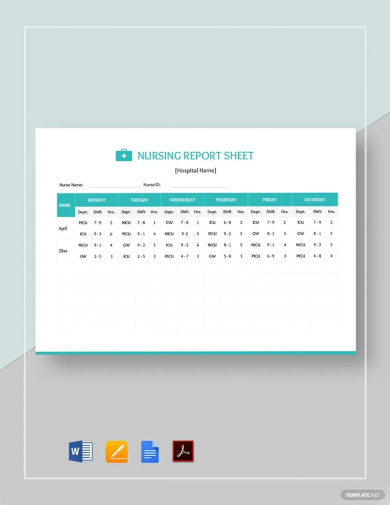
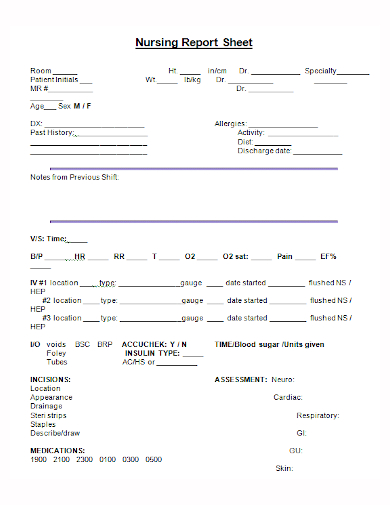
1. Nursing Report Sheet
2. Free Nurse Report Sheet
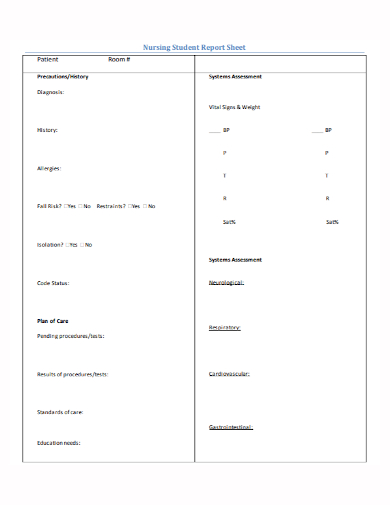
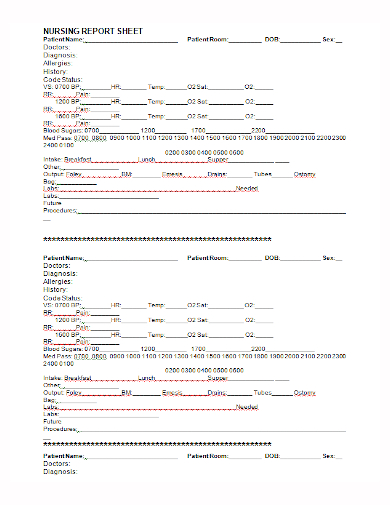
3. Nursing Report Sheet PDF
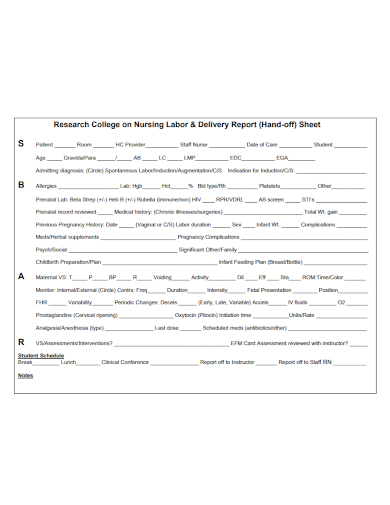
4. Nursing Labor And Delivery Report Sheet Free
5. Nurse Report Sheet Printable
What are nursing notes of patients?
Nursing notes, also known as progress notes or nurses’ documentation, are written or electronic records that nurses maintain to document patient care activities, observations, and interventions during their shift. These notes include vital signs, medication administration, changes in patient condition, responses to treatment, and any other relevant information. Nursing notes serve as a crucial communication tool among healthcare providers, ensuring continuity of care and facilitating collaboration within the healthcare team. These records are legal documents that contribute to a patient’s overall medical history, aiding in clinical decision-making, quality improvement, and ensuring accountability in nursing practice.
6. Nursing Report Sheets
7. Free Printable Nursing Report Sheet
What is nursing assessment sheet?
A nursing assessment sheet is a structured document used by nurses to gather comprehensive information about a patient’s health status, medical history, and current condition. This sheet is a fundamental tool in the nursing process, providing a systematic approach to collecting and organizing data that informs the planning and delivery of patient care. The content of a nursing assessment sheet may vary, but it typically includes the following components:
- Patient Information: Demographic details, including name, age, gender, and contact information.
- Chief Complaint: The primary reason the patient is seeking medical attention or hospital admission.
- Health History: Comprehensive information about the patient’s past and current health, including medical conditions, surgeries, allergies, medications, and family history.
- Vital Signs: Recording of the patient’s vital signs, such as temperature, heart rate, respiratory rate, blood pressure, and oxygen saturation.
- Physical Assessment: A systematic examination of the patient’s body systems, including neurological, cardiovascular, respiratory, gastrointestinal, musculoskeletal, and integumentary assessments.
- Psychosocial Assessment: Evaluation of the patient’s mental health, emotional well-being, support systems, and coping mechanisms.
- Pain Assessment: Documentation of the patient’s pain levels, location, duration, and any factors that alleviate or exacerbate pain.
- Nutritional Assessment: Information about the patient’s dietary habits, nutritional status, and any specific dietary restrictions.
- Activities of Daily Living (ADLs): Assessment of the patient’s ability to perform self-care activities, such as bathing, dressing, eating, and mobility.
- Diagnostic Tests and Results: Documentation of any diagnostic tests conducted, including laboratory results, imaging studies, and other diagnostic procedures.
- Medication History: Details about the patient’s current medications, dosage, frequency, and any adverse reactions.
- Nursing Diagnoses: Identification of actual or potential health problems based on the data collected, which guides the nursing care plan.
Nursing assessment sheets serve as a crucial communication tool among healthcare professionals, ensuring that all members of the healthcare team have access to essential patient information. This comprehensive document aids in the delivery of safe, effective, and patient-centered care.
8. Printable Nursing Report Sheet PDF
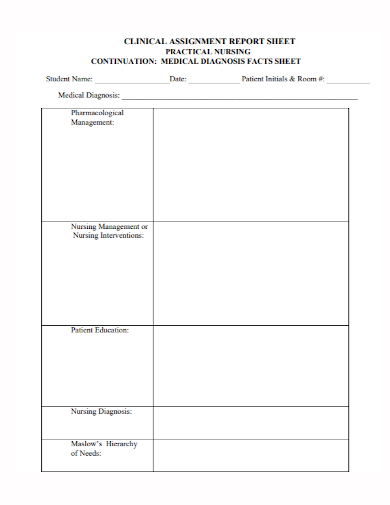
9. Nursing Clinical Report Sheet Format
10. Nursing Shift Report Template
11. Simple Nursing Report Sheet
12. Nursing Report Sheet Template Free
Making this Nurse Report may be hard to do if you are new in the field or you are not a practitioner of the said responsibility. Nevertheless, having this readily at hand will help you better understand the field nurses are in, this could also help you realize why these nurses ask a lot of questions every now and then. You don’t need to worry about anything, you are safe in their hands.
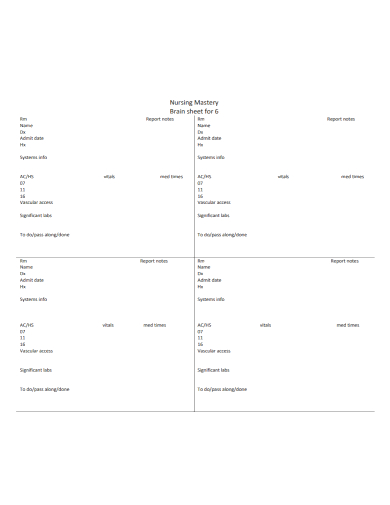
What is a Nursing Brain Sheet?
A nursing brain sheet is a structured document that nurses use to organize and record essential patient information during their shift. It typically includes sections for vital signs, medications, procedures, and other key details, serving as a quick reference for efficient and comprehensive patient care.
What Is A Nurse’s Brain?
If you happen to be a Nurse, a Nurse’s Brain for your patients will help you better prioritize your day and keep in track all the relevant information that you need to finish for the day. You might want to come in early to research patients, check their conditions and sample plan your day, so you can fill out some of this info before you get a report from the previous nurse as the oncoming nurse that is assigned for the next shift.
It can also help you give more effective reports sample to your oncoming nurses for the next shift or to a doctor if asked or if needed. If you learn to do this very well, especially if you are a practitioner in field, your coworkers and other professionals involving in the medical institution you are in will respect the care and organization you put in to making their lives easier, which will improve nursing relationships with those coworkers. It also helps you take better care of your patient’s health by constantly being updated with their conditions — because you are more organized and can clearly communicate what you need from the doctor, or oncoming nurse by using this simple yet very important piece of paper.
Using Your Nurse’s Brain To Coordinate With The Oncoming Nurse
At the end of your nursing shift, you need to allot a reporting time to give a comprehensive update of information to the oncoming nurse. During this transfer of responsibility and duties, the oncoming nurse needs to know the most important information about your patients, so it’s your job to give a concise, understandable, utilizable and organized report on each of the patients under your care. The amount of time management you have for each patient’s report depends on where you work and the nurse to patient ratio, but it’s usually around 5 minutes per patient, it also depends on the patient’s condition, the severe of the condition is, the more time required for follow ups and checking.
Your Nurse’s Brain can function as a nursing handoff report template, too, just so you know. If you have kept track of this information using your Nurse’s Brain, it’s easy to quickly transfer the knowledge at shift change, and it could help the other nurses to do better just by following and keeping track of your records.
FAQs
1. What is the purpose of Nursing Report?
Report summary the services of the nurse and/ or the agency. Reports may be in the form of an analysis of some aspect of a service reports. These are based on records and registers and so it is relevant for the nurses to maintain the records regarding their daily case load, service load and activities.
2. Do nurses have to write a lot?
The field of nursing requires a great deal of swift, accurate writing. You will need to fill out reports and charts correctly and completely and record your interactions with doctors and patients fairly. In addition, you must always be prepared to defend the information you record.
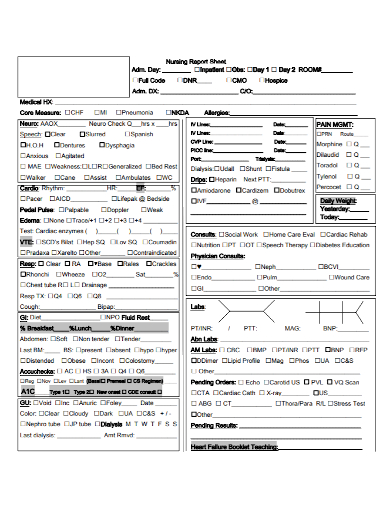
3. What is a nurse report sheet?
A nurse report sheet is a document used by nurses to organize and convey essential patient information during shift handover report. It typically includes details about patient care, vital signs, and tasks.
4. How do you take a nursing report?
When taking a nursing report, actively listen, ask questions for clarity, and note critical patient information. Focus on medical history, current status, treatments, and any upcoming interventions or concerns.
5. What is report writing in nursing?
Report writing in nursing involves documenting patient assessment form, interventions, and outcomes. It ensures clear communication among healthcare professionals, maintaining accurate and comprehensive records for continuity of care and accountability.
6. How do you make a brain sheet for nursing?
Create a nursing brain sheet by organizing patient information into clear sections such as vital signs, medications, procedures, and notes. Customize it to suit your sample workflow, facilitating efficient patient care.
In conclusion, this nursing report encapsulates the patient’s holistic care journey, detailing assessments, interventions, and outcomes. It stands as a valuable document, facilitating continuity of care and informed decision-making. The dedication of healthcare professionals is evident, emphasizing the commitment to patient well-being and quality healthcare delivery.
Related Posts
FREE 36+ Incident Reports
FREE 22+ Sample Incident Report
FREE 13+ Tutor Evaluation Form Samples
FREE 10+ Hospital Incident Report Samples
FREE 10+ IT Assessment Templates
FREE 9+ Sample Incident Reporting Forms
FREE 7+ Sample Time Management
FREE 6+ Staffing Model Samples
FREE 6+ Sample Nursing Assessments
FREE 33+ Budget Templates
FREE 11+ Sample Career Assessment
FREE 10+ Workload Analysis Samples
FREE 10+ Chronic Care Management Samples
FREE 9+ Sample Need Assessment
FREE 8+ Nursing Assessment Samples